Mako robotic-arm assisted anterior total hip replacement surgery is cutting edge technology that provides each patient with a personalized surgical plan based on the unique anatomy of their hip. It has been developed in the United States and has been introduced to Australia. Dr Limbers is one of the first surgeons in Australia to use this technique.
Total hip replacement is a procedure designed to relieve pain caused by joint degeneration due to osteoarthritis of the hip, by replacing the worn-out ball and socket joint with prosthetic components. Mako robotic technology provides Dr Limbers with a patient specific 3-D model to pre-plan your total hip replacement. During surgery, he guides the Mako robotic-arm based on your patient-specific plan. This allows him to remove only the diseased bone, preserving healthy bone and soft tissue, and assists him in positioning the implant based on your anatomy.
Prior to surgery a CT scan of your hip is performed and is used to generate a 3D virtual model.

This virtual model is loaded into the Mako system software and is used to create your personalized pre-operative total hip replacement plan.
In the operating room, Dr Limbers performs a minimally invasive anterior approach to your hip joint. This technique approaches the hip joint in an intermuscular plane, ensuring that no muscles are divided. This has been shown to have less pain in the first 6 weeks after surgery and accelerated rehabilitation, without the traditional post-operative hip precautions. He inserts navigation pins into the pelvic bone above the hip. He then maps the anatomy of your hip joint. All this information is detected by a specialised camera and passed to the Mako robotic unit. The surgical plan is then adjusted based on this additional information obtained during surgery. The robotic unit then guides Dr Limbers within the pre-defined area while he prepares the acetabulum (hip socket) and femur (thigh bone) to take the hip replacement components.
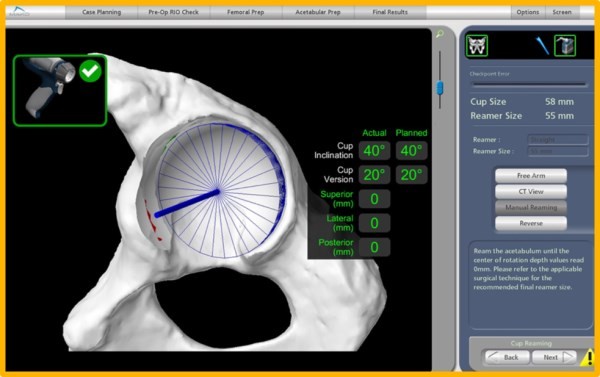

After the bone preparation Dr Limbers implants the metal acetabulum and femoral components with a ceramic femoral head and a polyethylene or ceramic acetabular liner between the components. The tactile, auditory and visual feedback of the robotic arm limits the bone preparation to the diseased areas and allows real time adjustments. This technique provides highly accurate placement and alignment of the components of the total hip replacement. This potentially results in a lower incidence of leg length inequality and a reduced chance of post-operative hip dislocation. It has the potential to improve long term results of total hip replacement surgery, by ensuring optimal implant position.
At the end of the procedure local anaesthetic is injected into the wound for pain relief. A local anaesthetic infusion catheter is also left in the wound to control pain. The wound is closed and covered with a waterproof dressing.
Hospital stay is usually 3 – 4 days. After that you will be discharged home or to a rehabilitation hospital. Most of the recovery is achieved in the first 6 weeks, with improvement continuing over 3 to 6 months. There is no restriction in hip movements or sleeping position in the first 6 weeks after anterior total hip replacement surgery. Driving is allowed after 4 weeks.
Is Robotic Joint Replacement Technology of Benefit to Patients?
Robotic unicompartmental (partial) knee replacement surgery was the first robotic joint replacement platform to be developed. The rationale was that unicompartmental knee replacement could particularly benefit from the increased accuracy, given the higher failure rate of conventional unicompartmental knee replacement when compared to total knee replacement. Short term data of robotic partial knee replacement has been presented showing a lower incidence of premature failure, when compared to traditional instrumented partial knee replacement techniques.
The acetabular cup placement was examined in robotically assisted and conventional total hip replacement surgery in a comparative study. A statistically significantly higher number (30% higher) of acetabular cups were positioned within the desired range of anteversion and inclination in the robotically assisted cases. Whether this translates into lower revision rates and increased patient satisfaction remains to proven.
Thus, the early data for robotic unicompartmental knee replacement and robotic total hip replacement is encouraging.
For Patients
Conditions
Procedures
Google Rating
4.8
Based on 189 reviews

Dr John Limbers | Orthopaedic Surgeon
4.8

Greg Gleeson
1775518052
Had a total left hip replacement( Anterior) six weeks ago. Wonderful result have full range of motion with no pain or restriction.
At 87 years of age could not be happier with this result.
Cannot speak highly enough of Dr. Limbers have no hesitation in recommending him.
At 87 years of age could not be happier with this result.
Cannot speak highly enough of Dr. Limbers have no hesitation in recommending him.

Paul Smith
1775097151
Had my right total knee replacement by Dr Limbers on 16 February 2026. From my initial consultation with him to the surgery and post op reviews, I cannot speak highly enough of his professionalism, communication and, particularly his skills. My surgery went like clockwork, the scar is hardly visible and the rehabilitation at Gosford Private was excellent. I was up and walking in no time and able to go home after two and a half days. I am now relatively pain free, not needing any pain medication, sleeping like a rock, walking unaided and back doing my favourite exercise, swimming. I can highly recommend Dr Limbers for anyone needing to undertake this surgery.

Tuff Buckets
1775088596
Mick Turner exception service i had a double knee replacement and very happy with my results

David Isaac
1774476172
Having researched surgeons for my hip replacement and preferring not to travel to Sydney, Dr. John Limbers was a standout for the Central Coast. Being aware that robotic assisted anterior hip replacement where possible, had benefits, I consulted with John. From the time I met John, I was impressed by his candor and knowledge. His willingness to address any concerns I had was reassuring. The subsequent operation and post operative care has been exceptional. I would highly recommend Dr. John Limbers to anyone considering hip surgery. I am now five weeks post operation, and pain free with excellent mobility.

Thomas Southwood
1773364302
Dr John Limbers , my wife Cora Anne had a total knee replacement early February 2026 , following this surgery and physiotherapy , Cora Anne is delighted with the outcome. Dr. Limbers was very easy to talk to & has a wonderful bedside manner. We recommend Dr. John Limbers to anyone looking for the best in his field

Wendy Vittorino
1771917800
Dr limbers performed an extremely successful total knee reconstruction for me 16 years ago, so I knew exactly the person I needed to perform my total knee replacement for my other knee . His work is impeccable. Scars are kept to a minimum and incredibly neat. He is friendly, informative and between him and his team are always there to answer any questions or address any concerns you may have. I have no hesitation in recommending Dr John Limbers to anyone who is wanting a fast recovery with fabulous post surgery results. At only 6 weeks post op im now out of pain and walking without any aids. He realigned my leg so it is straight again and my tendons are tracking smoothly. At only 48 years old I wanted the best outcome as I still have many active years ahead of me and I definitely have recieved that!!

Craig Westren
1769492019
I have no hesitation in recommending Dr John Limbers for any orthopaedic requirements. I have just had my final clearance from Dr Limbers after having a bilateral hip replacement. The surgery went perfect and I could not believe how fast the recovery was. I only used crutches for a week then a walking stick for another week then I was walking perfectly unassisted. It’s now 6 weeks post op and I feel 10 years younger not one bit of pain.

Michael Lord
1769217664
Without a doubt John is an extremely talented and skilled surgeon. Starting with how he does his incision to the side of the knee (compared to most who cut straight down the middle), to his choice to operate with the Stryker Mako assisted robotic arm and using Stryker Triathlon Tritanium Implants.
I'm 6weeks post operation of a total knee replacement, walking 5km at a normal pace. Minimal to no pain after just a couple of weeks
I believe this is due in most to John's skills and his choice of proceed & components.
If you are in the need of an Orthopaedic surgeon, you could do no better than to talk to John about what you may require. His advice is delivered in a straight forward, well explained manger which provides the confidence that you want to under go this procedure.
I'm 6weeks post operation of a total knee replacement, walking 5km at a normal pace. Minimal to no pain after just a couple of weeks
I believe this is due in most to John's skills and his choice of proceed & components.
If you are in the need of an Orthopaedic surgeon, you could do no better than to talk to John about what you may require. His advice is delivered in a straight forward, well explained manger which provides the confidence that you want to under go this procedure.

Gail Ash
1768614440
I was fortunate enough to have Dr Limbers as my hip surgeon 12 months ago in January 2025. A wonderful surgeon who put me at ease, and I couldn't recommend him highly enough. He's also a lovely man who builds great rapport with his patients. 12 months on after a hip replacement, I couldn't be feeling better. Thank you Dr Limbers!


Kathryn Edwards
1766438994
I have had such a positive outcome for my bilateral knee replacements. I’m 5 weeks post op and my recovery has been amazing. Thankyou Dr. Limbers for the professionalism and giving me the confidence that I would have this positive outcome.

Guy Ellis
1766016422
If you have a need for a Orthopaedic surgeon. This bloke is the best in the business. I have just had total hip replacement by him and his team. He uses the latest technology with robotics. I couldn't not be happier with the results.

Dummy Email
1765251630
A very good and successful Orthopaedic experience with Dr Limbers. I had a total hip replacement with Mako after years of suffering Osteo arthritis. I'm very comfortale now after only 6 weeks post Op, thankyou to Dr John Limbers and team at Gosford private hospital.

Matt Sweetnam
1765161599
My total right knee replacement has been a fantastic experience. With the expected pain and discomfort aside, the recovery from sugery has been fantastic. From start to finish, everyone with Dr Limbers team have been absolutely outstanding-nurses and physios included. In the coming weeks I expect to recover further and will be eternally grateful for the opportunity to have this surgery. Thanks Dr Limbers and your Team.

chris Kokegei
1763100437
Recently I was very fortunate to be referred to Dr John Limbers with major problems with my left hip. After a very thorough examination and study of my scans and X Rays Dr Limbers proposed a full hip replacement and ceramic insert. He explained the whole process in an easy to follow manner including all post operative treatments. Tomorrow it will be 6 weeks post surgery, Wow, amazing, unbelievable are some words that come to mind !
I find it hard to believe how much I have improved so much, so quickly and almost zero pain. I am walking without aids and I haven't felt this good in years. His staff and all those at Gosford Private Hospital were also amazing with their care and support, prior to operation, during hospital and Exercise Physiologists Post Op rehabilitation. I cannot thank him enough, I only wish I had done it sooner. If you want Terrific care from a Professional, Caring and Dedicated Team then call Dr.John Limbers now !!!
In March 2025 I needed a full knee replacement and once again I was fortunate to have my surgery done by Dr.John Limbers and his team at Gosford Private Hospital.
As previousley stated, the care, professionalism and support from Dr. Limbers and his whole team was amazing. I knew in advance what to expect in terms of pain and post operative management. They were so incredibly thorough and supportive
Pre op, during hospitalisation and Post operative treatment.
I cannot thank Dr.John Limbers and his team enough and would not hesitate to recommend them to anyone who is experiencing
joint and mobility issues. If you are suffering then call Dr Limbers
immediately and make an appointment, you will be so glad you did !!!
From
; Chris Kokegei an eternally grateful patient.
I find it hard to believe how much I have improved so much, so quickly and almost zero pain. I am walking without aids and I haven't felt this good in years. His staff and all those at Gosford Private Hospital were also amazing with their care and support, prior to operation, during hospital and Exercise Physiologists Post Op rehabilitation. I cannot thank him enough, I only wish I had done it sooner. If you want Terrific care from a Professional, Caring and Dedicated Team then call Dr.John Limbers now !!!
In March 2025 I needed a full knee replacement and once again I was fortunate to have my surgery done by Dr.John Limbers and his team at Gosford Private Hospital.
As previousley stated, the care, professionalism and support from Dr. Limbers and his whole team was amazing. I knew in advance what to expect in terms of pain and post operative management. They were so incredibly thorough and supportive
Pre op, during hospitalisation and Post operative treatment.
I cannot thank Dr.John Limbers and his team enough and would not hesitate to recommend them to anyone who is experiencing
joint and mobility issues. If you are suffering then call Dr Limbers
immediately and make an appointment, you will be so glad you did !!!
From
; Chris Kokegei an eternally grateful patient.

John
1763029064
I had both hips replaced and was walking without assistance in the second week. I used a walker for my own security but didn't need it.


John S
1761103480
Since my review below, back in March '25, I have had a partial replacement on my LH knee in early August. I was walking with a frame next day and then without any form of assistance on the second day after the operation. After 9 years of increasingly reduced outdoors mobility, I feel at least 10 years younger. My knees have no constraints on flexibility or speed of walking and no pain in moving or kneeling.
As in my earlier review below, I feel an enormous debt of gratitude to John Limbers for his technical skill and an outcome beyond my expectations. On top of this, his daily contact and reassurance along with meaningful follow up after discharge make him someone I would recommend without any reservations at all.
Since I had experienced periods of strong RH knee pain starting 8 years ago, which had steadily increased in discomfort until 7 weeks ago, I finally had a full knee replacement performed by the incredible Dr John Limbers and his team at the SAN hospital at the end of February.
I was home 6 days later, able to use the stairs with just the rail for assistance (3 storey home) and not needing crutches from day one. It has been a day by day improvement in mobility since then. Surgical discomfort from exercising has only required a reducing Panadol intake for the last 3-4 weeks.
Without any doubt John Limber's huge experience, skill level with the Mako procedure and ability to communicate and reassure, have given an outcome which is completely satisfying to both me and my family.
As well, on top of his obvious surgical skills he is both a gentleman and a caring individual.
As in my earlier review below, I feel an enormous debt of gratitude to John Limbers for his technical skill and an outcome beyond my expectations. On top of this, his daily contact and reassurance along with meaningful follow up after discharge make him someone I would recommend without any reservations at all.
Since I had experienced periods of strong RH knee pain starting 8 years ago, which had steadily increased in discomfort until 7 weeks ago, I finally had a full knee replacement performed by the incredible Dr John Limbers and his team at the SAN hospital at the end of February.
I was home 6 days later, able to use the stairs with just the rail for assistance (3 storey home) and not needing crutches from day one. It has been a day by day improvement in mobility since then. Surgical discomfort from exercising has only required a reducing Panadol intake for the last 3-4 weeks.
Without any doubt John Limber's huge experience, skill level with the Mako procedure and ability to communicate and reassure, have given an outcome which is completely satisfying to both me and my family.
As well, on top of his obvious surgical skills he is both a gentleman and a caring individual.

john hickey
1760413351
First thing doctor limbers said to me at first consultation was let’s give you a better life and that’s exactly what him and his team did ,it’s been 8 weeks since having both orthopaedic knees done and walking free of pain after 3weeks , I was recommended by numerous people about this outstanding surgeon and they where exactly right , cheers

Samantha Robinson
1759467108
I had a hip replacement in April and cannot say enough positive things about my experience, from the support staff, the anaesthetist and obviously the surgeon - Dr Limbers. I had the operation on the Thursday and was out and at home on the Friday. My recovery was steady and I was amazed at how soon it was a case of "what hip?" when peopled asked about my hip replacement. Dr Limbers is an incredible surgeon who has given me back my physical freedom. I am now doing things I was unable to do for around 8 months as a result of his skill. I would highly recommend Dr Limbers who takes a keen interest in your recovery and ensuring that you are up and at it soon after the operation to support that strong recovery. I hope my other hip doesn't need a replacement, but if it does, I will be straight back to Dr Limbers for that operation. Many thanks to him and his team, who were responsive and always ready to answer any questions that I had. They're all amazing.

Sue Bradley
1759229689
It has been just 8 weeks since I had a full hip replacement. I am amazed at the progress and movement I have - Dr Limbres right from my first meeting with him has been exceptional, he explains everything so well, so professional and with care, the whole experience on surgery day I couldn't fault, the team were wonderful. From my first step to weeks following post surgery, the supports at North Gosford were fabulous. I did my research on surgeons, and found Dr Limbres to be very experienced, used up to date technologies and even consulted with other pier surgeons, as mine was a little different being hip dysplasia and went so far as to accommodating my requests by understanding my concerns and really listened. I highly recommend Dr Limbres I have a renewed lease on life that I will be forever grateful.

Noel McMaster
1758962645
To Dr Limbers and his amazing team thank you so so much. With cancer making my hip surgery not so straight forward. I am forever grateful. Never thought I would ever be this pain free and moving so freely. Thanks again 10/10
Noel McMaster
1758959724
Thought I was never going to be out of pain with my hip due to complexed medical issues having cancer. To Dr Limbers and his amazing team thank you. I am a new man pain free.

Donna Chan
1758866625
Dr. Limbers replaced my right hip in 2024 and then my left hip in 2025 using the Mako robotics assisted anterior surgery. The results are excellent. The recoveries for both surgeries have been smooth and easy. This second time around I was able to walk and go up and down the stairs without any aid after 5/6 days. I am now free of any pain and can carry on my life.
Thank you Dr. Limbers!
Thank you Dr. Limbers!


Col Mathews
1757452956
I can highly recommend Dr Limbers to anyone in need of his services. He carried out both a knee and hip total replacement on myself and have been extremely happy with the results and recovery process. It has added value to my life in mind, body and spirit

Andrea OH
1756502703
Great experience with Dr Limbers after hip replacement surgery. Up walking the next day and without crutches inside week 1, very experienced team and certainly five stars.

Graham Harris
1756437467
After putting off a hip replacement for near on 4 years and consulting with a few surgeons I was recommended Dr John Limbers. I ended up having a Mako assisted anterior hip replacement with Dr Limbers and going on week 5 from the surgery I am extremely pleased with the results. The pain I experienced for years is close to completely gone and my ability to move, walk and do the things I love is getting better and better every day. I should probably have had this done sooner, but I am also glad I did not and ended up with John who is a straight talker, passionate about what he does and a great surgeon. I highly recommend him.

Richard Gooderham
1756429391
Dr.John Limbers was great from start to finish in terms of his explanation of the procedure and recovery. Certainly having a great surgeon using the latest technology to ensure best possible outcome for me his patient. Very happy 7 weeks post surgery with the bilateral total knee replacements and I would recommend John if looking for new knees!. Important you do your rehab!

Pam Austin
1754266785
Had right hip replacement late February. Dr Limbers very professional. Visiting each day at hospital which diosnt happen much these days. The best outcome with my hip up and about no trouble. Recommend doctor Limbers highly

LEILANI BRAASCH
1753938338
Dr Limbers has replaced both my knees. The first in 2019 and 7 weeks later I was on a walking holiday in Vietnam with no problems at all. The second knee was replaced in January 2025 (I'm 68) and in May I went on a walking holiday in various parts of Europe. I was able to do all the walks and not once did I have any problems with my knee. I love walking and he gave me back that enjoyment both times. I highly recommend Dr Limbers

Margarette Adams
1753927630
Dr Limbers performed a Total knee Replacement on my left knee 5 weeks ago . He is very professional and caring through the whole process starting with the first consultation, the surgery and post surgery care. I can not be more happy about the outcome. Less than 6 weeks after surgery I am walking and swimming and getting back to my life again after having months of pain and limping. I would strongly recommend Dr Limbers and his team without any hesitation.

Penny Brenton
1753326404
I’m so delighted with my new knees! 😁
Dr Limbers replaced both my knees on 30/1/25.
6 months later I have zero pain and exceptional mobility and flexibility in both knees.
Dr Limbers, I couldn’t be happier or more grateful…. Thank you 🙏🏻
Anyone considering knee replacement surgery, I highly recommend Dr Limbers.
His staff are also super nice and extremely helpful, even organising my health fund rebate post surgery for me.
They’re a fabulous team. 🙏🏻🙏🏻
Dr Limbers replaced both my knees on 30/1/25.
6 months later I have zero pain and exceptional mobility and flexibility in both knees.
Dr Limbers, I couldn’t be happier or more grateful…. Thank you 🙏🏻
Anyone considering knee replacement surgery, I highly recommend Dr Limbers.
His staff are also super nice and extremely helpful, even organising my health fund rebate post surgery for me.
They’re a fabulous team. 🙏🏻🙏🏻

Baumeister pty/ltd Master Builder Gerrit Duits
1751450252
Dr.John Limbers is nothing short of an absolute Master; he is more than Outstanding as a Specialist and Educator.
I am deeply honoured to provide this long-overdue reference for my great friend and exceptional orthopedic surgeon, Dr. John Limbers.
In my experience,
Dr. Limbers is one of the country's most dedicated, caring, and skilled professional orthopedic surgeons.
His Exceptional Skills and Knowledge are unmatched.
As a patient, I have witnessed Dr. Limbers' exceptional skills firsthand. His lectures to a broad audience of professionals, including my esteemed friends and Laureate Medical Professors,
John has consistently demonstrated his love, knowledge, and abilities far beyond exemplary.
Unwavering Commitment👈
Dr. Limbers' dedication to his craft is inspiring. His commitment to delivering outstanding results is evident in every aspect of his work. His skills and knowledge have significantly impacted my life, particularly regarding my knee and wrist surgeries.
100% Functionality Regained
Thanks to Dr. Limbers' love, dedication, and expertise, I have regained 100% functionality in my knee and wrist. His professionalism, care, and attention to detail are truly exceptional.
A Legend in His Field
Dr. John Limbers is a legend in his field, and I am not alone in my admiration for his work. His contributions to orthopedic surgery are invaluable, and I am grateful for the opportunity to work with him.
Conclusion
If I were to win ten million dollars today, I would still be back at work tomorrow. However, I would be eternally grateful for the exceptional care and expertise that Dr. Limbers has provided. Thank you, Dr. Limbers, for being an outstanding surgeon, educator, and professional.
Warm regards,
Gerrit Duits
Baumeister Pty Ltd
I am deeply honoured to provide this long-overdue reference for my great friend and exceptional orthopedic surgeon, Dr. John Limbers.
In my experience,
Dr. Limbers is one of the country's most dedicated, caring, and skilled professional orthopedic surgeons.
His Exceptional Skills and Knowledge are unmatched.
As a patient, I have witnessed Dr. Limbers' exceptional skills firsthand. His lectures to a broad audience of professionals, including my esteemed friends and Laureate Medical Professors,
John has consistently demonstrated his love, knowledge, and abilities far beyond exemplary.
Unwavering Commitment👈
Dr. Limbers' dedication to his craft is inspiring. His commitment to delivering outstanding results is evident in every aspect of his work. His skills and knowledge have significantly impacted my life, particularly regarding my knee and wrist surgeries.
100% Functionality Regained
Thanks to Dr. Limbers' love, dedication, and expertise, I have regained 100% functionality in my knee and wrist. His professionalism, care, and attention to detail are truly exceptional.
A Legend in His Field
Dr. John Limbers is a legend in his field, and I am not alone in my admiration for his work. His contributions to orthopedic surgery are invaluable, and I am grateful for the opportunity to work with him.
Conclusion
If I were to win ten million dollars today, I would still be back at work tomorrow. However, I would be eternally grateful for the exceptional care and expertise that Dr. Limbers has provided. Thank you, Dr. Limbers, for being an outstanding surgeon, educator, and professional.
Warm regards,
Gerrit Duits
Baumeister Pty Ltd

Rocco Versace
1747959161
After more than 12 months of hip pain, i had a hip replacement via the robotic assisted anterior approach. Dr Limbers is a wonderful surgeon who makes you feel very comfortable with all aspects of the surgery. He explains things very well and listens to your concerns. 6 weeks post op and i feel so much better, walking freely without pain. I highly recommend Dr Limbers and his staff to anybody who is in need of joint replacement.
Thanks to you and your staff Dr Limbers
Thanks to you and your staff Dr Limbers

Elaine Clancy
1747535876
Fantastic surgeon and experience. Was there in support pre and post operation and all the follow ups after. Would highly recommend to anyone needing a joint replacement procedure.

Linley Blayden
1746743646
After going for several months of pain and limited movement with my hip to having a total hip replacement by Dr John Limbers to having my active life restored.
I can recommend Dr Limbers and his staff to anyone needing hip replacement surgery to provide the best possible outcome.
I can recommend Dr Limbers and his staff to anyone needing hip replacement surgery to provide the best possible outcome.

Dee Thompson
1745911884
Just had total left robotic knee replacement and couldn’t be happier .. Dr Limbers is a very experienced surgeon who inspired me with confidence from day one. Everything was spelled out and no surprises, great after care and rehabilitation that started me on the right track for when I went home. His staff always at the end of a phone.
I cannot recommend him enough,if you’re looking for hip or knee replacement go to the best in my opinion.
Thank you Dr Limbers
I cannot recommend him enough,if you’re looking for hip or knee replacement go to the best in my opinion.
Thank you Dr Limbers

Andrew Krumm
1744270077
So pleased with my new hip, and have begun to resume an active, pain-free lifestyle. Thanks so much Dr Limbers.

Jennifer Hruby
1743198818
Dr John Limbers is an exceptional surgeon with excellent communication skills. His quiet confidence and manner put you at ease immediately. I had a Mako Robotic Hip Replacement seven weeks ago and couldn't be happier with the results. Operated on the Friday and home on Monday and by the end of the first week did not need any walking aid and PAIN FREE. Can't believe how fast I recovered. Dr Limbers is an amazing surgeon and his staff are always available with any questions you may have. I highly recommend this wonderful surgeon and wish I could give him 10 stars. Thank you Dr Limbers!

Helen Wood
1742340017
Dr Limbers and his team were very professional in all aspects of my MAKO TKR surgery. Now six weeks after surgery I have full use of my knee, walking well and have actually knelt without pain once.

lyn cappella
1742115089
10 weeks after hip replacement coming along well I found Dr limbers was caring and a great surgeon so glad he did my operation he is very caring and explained everything to me highly recommend

Helen Jones
1741917896
I did my due diligence and found Dr Limbers. I wanted an orthopaedic surgeon who practices the latest research based techniques. I now have a new total knee replacement and am so grateful for Dr Limbers and his team, they have given me my life back! Thank you from a retired registered nurse.

Yvonne Starkey
1738840020
I had a mid foot fusion in october 24 i would definatly recommend Dr Limbers he is so loverly and the Reception ladies are as well very caring and helpful

Janet Dixon-Hughes
1738758757
John Limbers is an excellent surgeon with excellent communication skills. I had a mako robotic total hip replacement at the SAN Wahroonga last September. Surgery Friday morning, walking with the forearm walker Friday lunchtime, walking with the normal walker in the evening, whizzing around the ward on Saturday, walking stick on Sunday morning, up and down the physio stairs at lunchtime and home Sunday afternoon. Pain gone. By Wednesday I was in the garden weeding. 3 Physio sessions were my total rehab. Walking stick gone in about 2 weeks. Doesn’t get better than that! 4 months later I am up and down ladders, gardening, renovating and back to things I hadn’t tackled in 10 years. Dr John is the best.

Michael Anderson
1723541596
Six weeks ago l had a consultation for a hip replacement. A big step for me, however, Dr Limbers and staff made it a worthwhile and speedy. Today l had my clearance to return to work No pain and no regrets. Great job Dr Limbers. Thanks hospital team and clinic staff.

Sue Densmore
1719358848
I’m 7 weeks post knee replacement and couldn’t be happier with my results. Dr Limbers and his team were very professional and caring. During my hospital stay Dr Limbers checked on my progress which was very reassuring. I have had minimal pain and the rehab provided at the hospital kept me on track for increased mobility and getting that bend. I highly recommend Dr Limbers.

Peter Whelan
1719291173
Dr John Limbers performed a total hip replacement 6 weeks ago. I can't speak highly enough of Dr Limbers professionalism, expertise and manner. Could not be happier with the outcome of the procedure.

Rod Hamilton
1719143018
Dr Limbers explained everything about the procedure beforehand. I am extremely pleased with the result of the hip replacement and would highly recommend him to others. Maxine Hamilton


Bella Eshman
1716266318
I recently had a bilateral knee replacement early April with Dr Limbers at Gosford Private. I am so thankful for Dr Limbers and my surgery. I am beyond happy with my outcome and the care and professionalism of Dr Limbers and his team. I thought it would be good after, but not this great and not such a quick amazing recovery. Giving 5 stars is just not enough. Natali Eshman

CORINNE Wheelwright
1715394476
6 months ago I had Robotic Bilateral knee replacements performed by Dr John Limbers at Gosford Private Hospital. From the initial appointment his care and knowledge of my situation was second to none. From not being able to walk without the aid of a walker and strong pain medication for severe pain, to walking without aid or medication and no pain, has given me my life back to perform my everyday activities. He is a life saver and a wonderful human being. Thank you Dr Limbers for giving me a second chance to getting my life back to normal.

Sam Buka
1714458108
After a few years of pain induced limping, I had both knees replaced by Dr Limbers. Within 2-3 weeks I was walking up and down stairs normally again without the assistance of the railing. Following rehabilitation physio, I am walking balanced, no limps, able to stand on one leg without fear of collapse. Pain free with newly regained mobility. Life begins again! I highly recommend Dr Limbers for expert treatment and care.

Tony Z
1713495106
Dr John Limbers performed a bilateral knee replacement on me in March 2024 and the result has been life changing. Gone is the constant knee pain and inflammation that plagued my every day life. I am able to walk pain free for the first time in more than two decades and cannot recommend him highly enough.

David Thorpe
1712780309
It is just 7 weeks since i had a double knee replacement. I was home in 6 days. i used a walking stick for 2 weeks. Had physiotherapy at North Gosford Private for 7 visits and was able to walk for 90 minutes unaided.
Dr Limbers is a very caring Surgeon and has done a fantastic job with my knees. I am now walking straight and i am no longer bow
legged. If you are wanting a new quality of life don't put it off.
Thanks Dr John.
Dr Limbers is a very caring Surgeon and has done a fantastic job with my knees. I am now walking straight and i am no longer bow
legged. If you are wanting a new quality of life don't put it off.
Thanks Dr John.

Peter Duckett
1712131330
When I found out I needed a Total Hip Replacement, I did my research on Orthopaedic Surgeons, particularly those on the Central Coast. Dr John Limbers name came up repeatedly, not only from acquaintances my age, who had the same operation but also from people who worked in the field. He came highly recommended. I have since had the other hip done by Doctor Limbers and I also have no hesitation in highly recommending him.

Tracey Thomas
1711682081
My mother had a knee replacement 8 weeks ago. She is doing incredibly well and very happy with the whole experience.

Stephen Tanko
1709324351
Dr John Limbers and his wonderful team gave a whole new meaning to the word professional. From day 1 in booking my initial appointment. I had a double need replacement in January, 2024. Dr Limbers and his team showed they are above and beyond the meaning of professional. The whole package was arranged pre- surgery, from pre-op X-rays referrals, pre- op medical test referrals, post op X-ray referrals and appointment with Dr Limbers 6 weeks post op. Dr Limbers assurance and brilliant skills with robotic surgery made my whole experience and outcome better than I thought possible. I don’t believe there is a better orthopaedic surgeon anywhere. Thank you again Dr Linbers and your staff.

Lewis Cini
1708590300
In 2017, Dr John Limbers
Gave me a double knee replacement, told me of all the risks ECT, and how long it would take me to heel.
I sincerely want to thank Dr John Limbers for giving me my life back.
Gave me a double knee replacement, told me of all the risks ECT, and how long it would take me to heel.
I sincerely want to thank Dr John Limbers for giving me my life back.

EC4U Office
1707457164
My Uncle Brian had knee reconstruction on 4th December with Dr Limbers and can not believe how quickly he has recovered relatively pain free.
Thanks for your amazing care and support
From the Mead Family.
Thanks for your amazing care and support
From the Mead Family.


Mary Wray
1703804054
Approximately 5 years ago I became aware of a problem with my left hip which slowly worsened over the following years until my GP referred me to Dr. John Limbars as he thought I needed an experts opinion of my condition. Within a short period of time after meeting with Dr. Limbers I was admitted to Gosford Private Hospital where surgery of the hip was performed. After the surgery the only discomfort I experienced was getting in and out of bed and in and out of our car which persisted for about 3 weeks becoming less painful as the days passed. After discharge from hospital where I received twice daily visits from the Physiotherapists I only had the need of a walking stick for about 2 more weeks . During this time I worked constantly on the exercises recommended by the Physios and at the end of the 3 weeks I was walking 1 km daily and spending time in our garden.
I can only praise Dr. Limbers for his expertise with the operation and wholeheartedly recommend his skills to anyone with hesitation about going ahead with this surgery.
However, I must mention here that my own perseverance following the recommendations from the physiotherapists helped with my recovery which after 6 weeks was excellent.
I can only praise Dr. Limbers for his expertise with the operation and wholeheartedly recommend his skills to anyone with hesitation about going ahead with this surgery.
However, I must mention here that my own perseverance following the recommendations from the physiotherapists helped with my recovery which after 6 weeks was excellent.

Troy van Buuren
1703118096
Consulted With Dr. Limbers on a Wednesday, got into meniscus surgery on the following Tuesday. Textbook recovery. Couldn't ask for any better. Dr. Limbers is highly professional, and showed a great deal of care from the beginning to the end of my case. Highly recommend!

Craig Allum
1701134659
Dr Limbers has done an amazing job on my hip. He was informative, personable and the quaility of his work has enabled me to do things after 6 weeks that i have not done in months. The recovery has been better than I could have expected and look forward to enjoying regaining full quaility of life back again. Super grateful to Dr Limbers and his team.

Phillip Jones
1699164025
I had a double knee replacement 3 months ago and and getting better every day. Dr limbers is a legend would recommend him to anyone!

Kerry Hunter
1698728826
Right knee replacement by Dr Limbers 5 years ago and left 6 weeks ago.
Extremely happy with the outcomes in both cases.
Dr Limbers is very caring surgeon.
Extremely happy with the outcomes in both cases.
Dr Limbers is very caring surgeon.

Greg Hawkins
1698263245
Sports, together with hard physical work and a family history of arthritis has resulted in damage to most joints in my body. Dr Limbers has undertaken ankle, and just recently a total knee replacement. Both of these procedures have been a total success, pain free, full movement returned enabling me to continue to participate in the activities that I enjoy the most. No doubt further procedures await me, I will have no hesitation in returning to John for these also.
I have no hesitation in recommending Dr Limbers to others, if I could give 6 stars I would!
I have no hesitation in recommending Dr Limbers to others, if I could give 6 stars I would!

Michelle Francis
1696483142
I have just had a double knee replacement with Dr Limbers. This is the second surgery he has performed on me-the first was a hip replacement last October. These two operations have given me my life back. I’m only 53 and therefore was worried about the knee surgery. I had lots of questions for Dr Limbers. He explained things brilliantly and reassured me throughout and he also dispelled several ‘myths’ regarding the surgery. For the first time in 25 years I can walk and stand without pain and the fear of my arthritic knees giving out on me. If you are living with constant pain don’t wait. Dr Limbers and the team at Gosford Private Hospital are professional, caring and determined to get the best result. I cannot recommend him highly enough.

Jane Apfel
1695425612
Excellent result from TKR ( total knee replacement) from Dr Limbers using the best of leading technology.
Brilliant result with excellent pain management.
If you think you need a TKR, do it now and don’t put it off. The sooner you get it done, the sooner you get back to your old life again.
Thank you Dr Limbers!!!
Brilliant result with excellent pain management.
If you think you need a TKR, do it now and don’t put it off. The sooner you get it done, the sooner you get back to your old life again.
Thank you Dr Limbers!!!

Ruth Cox
1694139714
Just reached the 7 week mark of having my 2nd knee replacement under Dr John Limbers. What an amazing experience, I was home within 5 days, basically pain free after nearly 4 months of constant pain. Now post rehab at the Gosford Private Hospital, I am almost back to normal, no walking aids since week 5 and a totally different experience to my first one. Dr Limbers and his staff have been amazing.

Owenn Spark
1693461745
Dr Limbers performed a total knee replacement on my left knee at Gosford Private hospital on 20/07/2023 . I was up on my feet the next day & came home on the 23/07/2023. I recovered at home quickly with the twice weekly physiotherapy & hydrotherapy sessions at the hospital. I have just done my first 6 weeks after my operation & ride my bike a few kms a day as well as walk about 3 km a day. The process is not pain free but manageable with only a small scar on the outside of my knee. Dr Limbers will definitely be the go to surgeon for my other knee when I need it replaced & have no hesitation in giving my 5 star rating. Yours Sincerely Owenn Spark

Roger Smith
1693377281
I am 100% happy with all the work he has done on me. I have had bilateral total knee replacements and a right hip replacement, and everything is working beautifully. I am 71 and I have a whole new lease on life, no longer hindered by the pain of walking. I thoroughly recommend Dr. John Limbers.

Elizabeth Whitelock
1690618694
Weeks post bilateral hip replacement and I have none of the excruciating pain I was experiencing. This gives me a new lease on life and I am forever grateful for the recommendation and Dr Limbers care.
I cannot speak highly enough of Dr Limbers’ extraordinary skill, patience, consideration and kindness.
I cannot speak highly enough of Dr Limbers’ extraordinary skill, patience, consideration and kindness.

Craig Brooking
1688107484
Dr Limbers has replaced both my hips and I am extremely happy with not only the results but also with the professional and friendly manner in which Dr Limbers dealt with me

Vicki O'Brien
1687931993
I am so greatful to John Limbers for the bilateral hip replacement
I have my life back pain free
You are amazing and your team eternally greatful
I have my life back pain free
You are amazing and your team eternally greatful

simon thorn
1687931001
Bilateral hip replacement on the 15th of may 6 weeks later I am over the moon at the results could not have asked for better.

Kelley Bennettt
1686566972
Dr Limbers performed a total knee replacement surgery on my right knee. His consultation provided me with all the information I needed to make an informed decision. From day 1 I have had minimal to no pain at all. I was up taking my 1st steps within 12 hours of arriving on the Ward & haven’t looked back. I am 7 weeks post surgery & life is almost back to normal. I would not hesitate to recommend Dr Limbers to anyone contemplating knee surgery.

Chris Varcoe
1686046735
Perfect surgery, great experience from John, ditched crutches on day 4 no pain relief required - would highly recommend

John Christoforou
1684231013
Great result. Now pain free. Dr Limbers has a great team, Anaesthetist, Nursing staff and physiotherapists. I could not fault the care and attention that I received.

Steve Field
1683775572
I would like to thank Dr John Limbers for my recent hip replacement surgery. I had been in pain and limited movement for over 2 years then finally went to Dr Limbers and after a short wait had the operation. It has been 7 weeks post op and I can already feel the improvement in movement and no more constant pain. Dr Limbers explains everything about the operation and the expected recovery time. His bed side manor is five star. Dr Limbers even rang my wife straight after surgery and explained how everything went.
Thanks Steve Field
Thanks Steve Field

Luke Burlet
1683596781
update - Mar 2023; now bilateral with other side done by Dr Limbers.
Since 3 years ago, Dr Limbers is much the same fellow per my comments below, maybe now even better. He has also improved his methodology with even more analysis of the lumbar and pelvic positioning w.r.t. the TRH to be done. Pretty impressive.
With the 2nd THR, so other side and am now bilateral, I was far more prepared physically and mentally; I'd strongly urge anyone getting THR to get a PRE-op plan from a physio, then about 2-3 weeks after surgery, do a POST-op plan with them. I did this time around, not the 1st, and the outcome after is even better. Per discussion with Dr L, I am about 6-7 wks ahead of 1st operation; back full time at gym 12 days after surgery, referring first grade u14 soccer (e.g. running) and have already booked winter ski trip with kids.
So all up, really successful two ops. If you have any concerns or any sort of questions do not be shy about asking Dr Limbers, he will carefully and wisely recommend options that are in your best interest.
Also should be noted his staff in Sydney office are very good; polite and prompt to answer any questions or concerns.
====
Dr Limbers did my TRH in Jan 2020.
I would 110% concur with all the 5/5 previous reviews; Dr John is not only a great surgeon but his 'bed side manner' at the referral, in surgery, immediate post-op check, and 6 week follow-up where exceptional. Don't get me wrong, you should choose a surgeon on skill and results but the non-tangible comes into it too. In my case, I am very technically oriented and cross check everything at work and home. No different here; I consulted three surgeons and although they were all good, Dr John out scored them not only technically but also on the human side so that I felt comfortable to ask technical and medical questions more than adequately. He listened carefully to not only my questions but also my suggestions for certain types of prosthetics that he happily gave me pros and cons for.
Another thing to consider - although Dr John is good he knows he can do better ... by using a robot (Mako) as part of the surgery; it assists in getting the position as correct as possible. He will explain better than I, but it is a no brainer that a technical or medical person should use the best tools available to them. If they can get better accuracy and a better result, costs considered, then why not use it? This was one of my main criteria was to find a surgeon that used a Mako robot to assist and get the 'replacement parts' put into the right angle, distance and length. I wanted as close as possible a natural result as I am young and do a lot of sports with my kids - Dr Johns achieved that in spades. I am very pleased.
Since 3 years ago, Dr Limbers is much the same fellow per my comments below, maybe now even better. He has also improved his methodology with even more analysis of the lumbar and pelvic positioning w.r.t. the TRH to be done. Pretty impressive.
With the 2nd THR, so other side and am now bilateral, I was far more prepared physically and mentally; I'd strongly urge anyone getting THR to get a PRE-op plan from a physio, then about 2-3 weeks after surgery, do a POST-op plan with them. I did this time around, not the 1st, and the outcome after is even better. Per discussion with Dr L, I am about 6-7 wks ahead of 1st operation; back full time at gym 12 days after surgery, referring first grade u14 soccer (e.g. running) and have already booked winter ski trip with kids.
So all up, really successful two ops. If you have any concerns or any sort of questions do not be shy about asking Dr Limbers, he will carefully and wisely recommend options that are in your best interest.
Also should be noted his staff in Sydney office are very good; polite and prompt to answer any questions or concerns.
====
Dr Limbers did my TRH in Jan 2020.
I would 110% concur with all the 5/5 previous reviews; Dr John is not only a great surgeon but his 'bed side manner' at the referral, in surgery, immediate post-op check, and 6 week follow-up where exceptional. Don't get me wrong, you should choose a surgeon on skill and results but the non-tangible comes into it too. In my case, I am very technically oriented and cross check everything at work and home. No different here; I consulted three surgeons and although they were all good, Dr John out scored them not only technically but also on the human side so that I felt comfortable to ask technical and medical questions more than adequately. He listened carefully to not only my questions but also my suggestions for certain types of prosthetics that he happily gave me pros and cons for.
Another thing to consider - although Dr John is good he knows he can do better ... by using a robot (Mako) as part of the surgery; it assists in getting the position as correct as possible. He will explain better than I, but it is a no brainer that a technical or medical person should use the best tools available to them. If they can get better accuracy and a better result, costs considered, then why not use it? This was one of my main criteria was to find a surgeon that used a Mako robot to assist and get the 'replacement parts' put into the right angle, distance and length. I wanted as close as possible a natural result as I am young and do a lot of sports with my kids - Dr Johns achieved that in spades. I am very pleased.

Noel Yule
1682549435
Dr. Limbers replaced my right knee just 7 weeks ago using the Mako robotic procedure which has allowed me to have an extremely speedy and comfortable recovery. I only required panadol to manage my 2 weeks of pain following my discharge from hospital.
Dr Limbers was once responsible for very successfully repairing my severed achilles tendon and now has done a superb job of giving me a new knee that will allow me to return to my sporting activities. He is an excellent surgeon , very thorough and most informative. I cannot thank him enough.
Dr Limbers was once responsible for very successfully repairing my severed achilles tendon and now has done a superb job of giving me a new knee that will allow me to return to my sporting activities. He is an excellent surgeon , very thorough and most informative. I cannot thank him enough.

Josef Rod
1681278050
Dr Limbers performed a Mako Robotic Total Hip Replacement on my left hip eight weeks ago . He is very professional and caring through the whole process starting with the first consultation, the surgery and post surgery care. I can not be more happy about the outcome. Less than six weeks after surgery I was walking, swimming and riding bicycle with no restriction or pain. I'm getting back to my life again after twelve month of pain and limping. I would strongly recommend Dr Limbers and his team without any hesitation.

martin barkl
1680075442
My recent hip replacement has been an astonishing success thanks to the skill of Dr Limbers. He is enthusiastic with well founded confidence, patient in answering questions and clear in his explanation of the process. Operation in the morning and on my feet the same afternoon, home a few days later. Pre and post physio is the key to making the most of the surgeon's skill.

Maureen Pancia
1679429628
6 weeks ago my husband who is 83 years old had a Mako Robotic Knee Replacement carried out by John Limbers. As he had had a previous knee replacement in Sydney 6 years ago done the conventional way we obviously were a little concerned but his explanation of the procedure convinced us. This type of surgery proved very successful he was up walking within 2 days and almost no pain management. Apart from the skills that Dr John has it was a pleasure to deal with a professional
and empathetic person. We can now venture onto our 3 month overseas trip in June Thank you Dr John!!
and empathetic person. We can now venture onto our 3 month overseas trip in June Thank you Dr John!!

Ruth Ah Sam
1678275655
Dr John Limbers carried out a very successful full knee replacement on my left leg in September 2022.
After having pain for many years and poor mobility I now live a pain free life and can walk long distances and exercise with great ease.
I am very thankful to Dr Limbers for turning my life around. 😊
After having pain for many years and poor mobility I now live a pain free life and can walk long distances and exercise with great ease.
I am very thankful to Dr Limbers for turning my life around. 😊

Noel Upcroft
1677648826
Fantastic result after 6 weeks bilateral knee replacements better already and more mobile than before the op very happy outcome cannot recommend any higher 👍👍

Andrew Parker
1674088398
Anterior total right hip replacement performed by Dr Limbers in November 2022. Was up and walking the next day (assisted) and unassisted 2 days later. Only spent 4 days in hospital....unbelievable! 2 month later, I am now living life completely pain free - riding my motorcycle, bushwalking & surfing. Would definitely recommend Dr Limbers

Mark Rasmussen
1674014332
I had my FKR 6wks ago and am over the moon painfree and totally loving my mobility. Thank you to Dr John and all the surgical staff and anaesthetist Dr Rielly who made my presurgery and post surgery a time to remember thank you

tracey peterson
1673003137
I had my double hip
Replacement surgery cancelled it March due to COVID 19
I had my surgery Rescheduled On 2nd July
I,m now home feeling so happy with everything
Dr limbers is a professional,I would not hesitate in using him again if needed
I,m up walking , I can actually stand up straight without kicking out my butt
The pain I had for last 2 years has completely gone , I,m so happy
With everything , I can’t wait untill I heal so I can get my life back
Just to walk without thinking about it is amazing , thankyou dr limbers and team ,having both hips done at same time is so worth it ..
Best regards
Tracey peterson
Replacement surgery cancelled it March due to COVID 19
I had my surgery Rescheduled On 2nd July
I,m now home feeling so happy with everything
Dr limbers is a professional,I would not hesitate in using him again if needed
I,m up walking , I can actually stand up straight without kicking out my butt
The pain I had for last 2 years has completely gone , I,m so happy
With everything , I can’t wait untill I heal so I can get my life back
Just to walk without thinking about it is amazing , thankyou dr limbers and team ,having both hips done at same time is so worth it ..
Best regards
Tracey peterson

Michael Hull
1671424104
Just hit six-week post op and I can't be happier with the results. Dr limbers from the initial appointment kept we well informed of expectations and the process. On the day of the surgery, he let me know what to expect again along with his team keeping me calm and aware of what was happening.
Post-surgery whilst in hospital he checked in regular on my progress. Along with the great post and rehab team I am back on the bike and have great flexion and returning strength.
I at some point will need my other knee done and I would not hesitate in going back to Dr Limbers.
Thank you for helping me return to a normal life.
Regard
Michael Hull
Post-surgery whilst in hospital he checked in regular on my progress. Along with the great post and rehab team I am back on the bike and have great flexion and returning strength.
I at some point will need my other knee done and I would not hesitate in going back to Dr Limbers.
Thank you for helping me return to a normal life.
Regard
Michael Hull

Rod Rogers
1671239577
Extremely pleased with Robotic hip replacement by Dr John Limbers on 4th Nov 2022.I was actually standing on my leg the next day with no pain and very little discomfort.John is very caring with delightful attitude and professionalism.Would totally recommend..

Denis Redfern
1671164462
Most people who decide to have a hip replacement don't know what they don't know about the long term implications of the different techniques used to perform the surgery. I was no exception. I feel very fortunate to have been referred to Dr Limbers. He uses a robotic-assisted direct anterior approach that does not involve cutting any muscles resulting in a much faster recovery and very few movement restrictions compared to posterior or lateral approaches. Six weeks on, I have no pain when walking or climbing stairs. I have no hesitation in recommending Dr Limbers and his team for this procedure.

Graeme Boman
1670893427
John was very professional and also very prompt with his services. I had both knees replaced and could not be happier with the result. Highly recommend !

Michelle Francis
1669959616
Dr Limbers was very professional. My hip surgery went without a hitch and the recovery was completely uneventful. Cannot recommend him (or his staff) highly enough.

Yvonne Mathews
1668475385
I am extremely pleased with the result from my hip operation performed by Dr John Limbers. Recovery was quick and the result fantastic. I have no hesitation in recommending him

David Oxley
1666065998
I must thank Dr Limbers for the excellent results from my recent Hip replacement. I am out of pain for the first time in 12 months.
Dr Limbers has such good communication skills, I was given a detailed explanation of what was going to happen pre & post operation.
The Robotic surgery left minimal scarring & physiotherapy has improved my flexibility.
It gets better each day thanks to the techniques used.
Thanks John, I look forward to a pain free journey ahead.
Dr Limbers has such good communication skills, I was given a detailed explanation of what was going to happen pre & post operation.
The Robotic surgery left minimal scarring & physiotherapy has improved my flexibility.
It gets better each day thanks to the techniques used.
Thanks John, I look forward to a pain free journey ahead.

karina bannister
1665553351
I would strongly recommend Dr Limbers, after he performed a total hip replacement for me. He was professional, explained the operation clearly and took the time to answer my questions and be considerate to my wishes prior to my surgery. 6wks post op and I have a great range movement with nil issues or concerns throughout my experience.

Eileen Darcy
1665359824
Excellent results having had both knees replaced robotically by Dr Limbers. Very professional, lovely bedside manner, and very reasonable out-of-pocket costs with private health fund contribution. Would highly recommend.

Kevin Bloor
1665292402
Dr Limbers did an excellent job replacing my left hip, the limp and pain that I tolerated before the surgery is well and truly a thing of the past.
The range of motion and relaxed muscles after only 8 weeks surprised my chiro. Even the leg length was the same for both legs. For years my pelvis was rotating as the left hip muscles tightened and the left leg shortened as a result of the pelvis rotation between chiro visits and this time pelvis hadn't rotated.
I am lucky that my GP referred me to Dr Limbers and strongly recommend Dr Limbers to anyone considering a hip replacement.
The range of motion and relaxed muscles after only 8 weeks surprised my chiro. Even the leg length was the same for both legs. For years my pelvis was rotating as the left hip muscles tightened and the left leg shortened as a result of the pelvis rotation between chiro visits and this time pelvis hadn't rotated.
I am lucky that my GP referred me to Dr Limbers and strongly recommend Dr Limbers to anyone considering a hip replacement.

Lynette Simunic
1663908526
Six weeks ago Dr Limbers performed a Mako Robotic Hip Replacement on me. I would recommend this amazing specialist to anyone. The whole time you are in his rooms, you are cared for, he is very relaxed and informative, and he listens to you. He is very approachable and very skilled. I have had the best possible outcome with my hip and the best care possible.
Financially Dr Limbers is very reasonable, and apart from his surgical skills , his bedside manner is very caring. Whilst I was in hospital he visited me and his other patients every day. I would highly recommend Dr Limbers. I would like to mention Dr Limbers surgical assistant Sr Leanne Flynn. I received a phone call from this lovely lady a few days after my surgery once I was discharged from hospital. Sr Leanne was concerned how my recovery was going and was very helpful with advice. Thank you very much Dr Limbers and your team.
Financially Dr Limbers is very reasonable, and apart from his surgical skills , his bedside manner is very caring. Whilst I was in hospital he visited me and his other patients every day. I would highly recommend Dr Limbers. I would like to mention Dr Limbers surgical assistant Sr Leanne Flynn. I received a phone call from this lovely lady a few days after my surgery once I was discharged from hospital. Sr Leanne was concerned how my recovery was going and was very helpful with advice. Thank you very much Dr Limbers and your team.

Steve P
1663714420
I had a knee replacement op. At six weeks, I am way ahead re recovery time/condition, and pain free (for the first time in years!). Cannot recommend John Limbers more highly (and it’s the general consensus when you ask those in the known in the area). Professional, very capable, and easy to talk to. I am grateful I went with John - Thank you very much.
Addition, one year later (September 2022): He did my other knee - same great result… that knee also doing very well no indeed. Can’t recommend Dr Limbers enough.
Addition, one year later (September 2022): He did my other knee - same great result… that knee also doing very well no indeed. Can’t recommend Dr Limbers enough.

Karyn Graham
1662018141
Dr John Limbers performed my knee surgery 6 weeks ago. I found him to be most attentive and caring. I would definitely recommend him.

Greg Al
1659530183
The recovery from the knee replacement procedure was very quick and with limited pain. A matter of 8 weeks from the operation I am back to almost full functionality in terms of normal daily activity and this continues to improve at a very rapid rate.
I would strongly recommend treatment by Dr Limbers for anyone seeking a knee replacemen.
I would strongly recommend treatment by Dr Limbers for anyone seeking a knee replacemen.

Philip Cassidy
1659081402
Several friends who had double knee replacements recommended Dr Limbers after great results. I am just sorry that I wasted 5 years before deciding on surgery. Whole process was not as intimidating as I had imagined and the results exceeded expectations. You are back on your feet before you know it. I can now resume a normal life walking, playing pickleball and enjoying my grandchildren.

Pat Athas
1656467686
I can thoroughly recommend Dr Limbers for any surgery you may require being hip replacement of which I have just experienced or knee replacement of which I know of persons with this procedure by Dr Limbers


Cliff Meecham
1653271349
I was recommended to see Dr John Limbers about my knee by a friend best advice I have ever had
I had put up with it for years I could only walk for five minutes then pain would kick in,Since having my knee replaced nine months ago I now have a great Quality of life back I’m 70years of age I am now walking ,working around the house ,all so woking casual as a bricklayers labourer , plus I’m back to playing Baseball and running bases freely, I have recommended DrLimbers to two of my friends who will now go to see him,
I thoroughly recommend Doctor John Limbers.
I had put up with it for years I could only walk for five minutes then pain would kick in,Since having my knee replaced nine months ago I now have a great Quality of life back I’m 70years of age I am now walking ,working around the house ,all so woking casual as a bricklayers labourer , plus I’m back to playing Baseball and running bases freely, I have recommended DrLimbers to two of my friends who will now go to see him,
I thoroughly recommend Doctor John Limbers.

Antony Schinckel
1651805896
Wonderful outcome of surgery for hip replacement - back on feet and home in a few days and very mobile extremely quickly. Minimal pain, no muscle issues. Anterior approach seems excellent for fast recovery

David McDowell
1644616195
John has done a knee replacement and 2 hips on me. All very successful.
I would like to recommend him as he gives first class services and follow up.
I would like to recommend him as he gives first class services and follow up.

Steve Martin
1643327386
I could not rate this doctor more highly. Dr Limbers gave me a knee replacement in 2018 and then a hip replacement in late 2021. I commented here on the knee replacement under the name of Steve Wotshisface. The more recent hip replacement was quite amazing. The surgery was completely successful and I am back to my usual life again. Most importantly, the recovery time was remarkably quick. My recovery was commented on by many medical staff. The physiotherapists were surprised at my quick recovery. A nurse during my hospital stay said very quietly to me "all of Dr Limbers patients seem to recover quickly." The pain management nurse/ doctor(?) was surprised at how little medication I required in the days following the surgery.
As with my knee post op, Dr Limbers was again actively interested in my recovery; not that there was much to do. I can only guess that the quick recovery is due to him being extraordinarily careful during the surgery.
The anesthetist working with Dr Limbers on both of my surgeries was Dr Coonan. Again, no problems at all and he was very careful in discussing my medical history before deciding what to do during the surgery. A really nice bloke as well.
From my experience I thoroughly endorse and recommend Dr Limbers, Dr Coonan, the San Hospital and their wonderful staff and I also recommend robotic surgery for hips and knees.
If you read this good luck with your surgery!!
As with my knee post op, Dr Limbers was again actively interested in my recovery; not that there was much to do. I can only guess that the quick recovery is due to him being extraordinarily careful during the surgery.
The anesthetist working with Dr Limbers on both of my surgeries was Dr Coonan. Again, no problems at all and he was very careful in discussing my medical history before deciding what to do during the surgery. A really nice bloke as well.
From my experience I thoroughly endorse and recommend Dr Limbers, Dr Coonan, the San Hospital and their wonderful staff and I also recommend robotic surgery for hips and knees.
If you read this good luck with your surgery!!

Sarah Broad
1643247370
Life changing! Explained exactly why a knee replacement was required and clearly explained the operation and recovery processes. Would absolutely not hesitate to have another replacement done on the other knee if required. Amazing experience, thank you John

Cheryl Cohen
1641771551
I had a full knee replacement by Dr Limbers in June 2021 which went extremely well.
I was pain free and walking without any aids within three weeks.
I felt very confident prior to the operation as Dr Limbers explained in detail how he would perform the surgery.
His admin staff are very pleasant and helpful to deal with.
I would highly recommend Dr Limbers and his team.
I was pain free and walking without any aids within three weeks.
I felt very confident prior to the operation as Dr Limbers explained in detail how he would perform the surgery.
His admin staff are very pleasant and helpful to deal with.
I would highly recommend Dr Limbers and his team.

Kevin Johnstone
1639704565
I am a retired Geriatrician. Unfortunately I suffered from bilateral hip osteoarthritis progressing to the stage that I was no longer able to ride my bike, mow the lawn or even walk my dog.
Dr John Limbers performed bilateral hip replacement surgery and the operation has truly changed my life.
I was out of hospital in 5 days, underwent rehabilitation at home and now 6 weeks later I have resumed all the above activities with minimal discomfort and continue to improve week by week.
His expertise and kindness has changed my life.
I will be forever thankful.
Dr John Limbers performed bilateral hip replacement surgery and the operation has truly changed my life.
I was out of hospital in 5 days, underwent rehabilitation at home and now 6 weeks later I have resumed all the above activities with minimal discomfort and continue to improve week by week.
His expertise and kindness has changed my life.
I will be forever thankful.

chris cassettari
1639473290
Dr John Limbers operated on my ankle a few months ago. I have suffered from inflammation and chronic pain for around 10 years after unsuccessful surgery from another surgeon.
My ankle has improved immeasurably. I can now walk with a straight leg. My hip pain has gone and my knee pain has reduced considerably. I am cross training, playing walking football and bush walking. I have more mobility and strength in my ankle than I have had in 15 years. My quality of life has increased and I hope to start running again in the new year.
Dr Limbers has a caring manner which I have not always found with specialist surgeons. I am very pleased to have chosen Dr Limbers for my surgery.
My ankle has improved immeasurably. I can now walk with a straight leg. My hip pain has gone and my knee pain has reduced considerably. I am cross training, playing walking football and bush walking. I have more mobility and strength in my ankle than I have had in 15 years. My quality of life has increased and I hope to start running again in the new year.
Dr Limbers has a caring manner which I have not always found with specialist surgeons. I am very pleased to have chosen Dr Limbers for my surgery.

Val Lumsdon
1635821921
I have just had my follow-up consultation with Dr Limbers after my second total hip replacement. I am so pleased to have found such a great orthopaedic surgeon. After suffering chronic hip pain for several years prior to my first surgery, I was amazed that I was virtually pain free immediately when I woke up from the anaesthetic. I therefore had no hesitation in making an appointment with Dr Limbers soon after experiencing pain in my other hip. Once again, I had no pain after the surgery and I am now able to live my life much the same as before the first surgery. Dr Limbers explained the procedure at the first consultation and has been very supportive throughout. I have no hesitation in recommending him to anyone suffering hip pain.

christopher colling
1635206509
When I knew it was time for a full hip replacement at 75yrs old I asked a friend, a nurse with many years experience in orthopaedic wards who they would recommend for my surgery. Dr. Limbers was there answer. I underwent robotic surgery on my right hip, spent 2 nights in Hospital and walked in my front gate on the 3rd day with the aid of only a walking stick. From that day on I had no need for pain medication. My 6 week return visit to Dr.Limbers showed excellent results and I was back on the road cycling the next day. My Nurse was right and Dr. Limbers gets 10/10 as a surgeon with a bedside manner as pleasant as the man himself.
Thanks Doc
ll Kind Regards Chris
Thanks Doc
ll Kind Regards Chris

Steve Martin
1631066810
A very good doctor. I had knee replacement surgery 3 years ago and it has been life changing. Dr Limbers has all the things you want in a surgeon; first and foremost he did a great job on the surgery; secondly I never felt abandoned in the post op care; and thirdly he showed kindness and compassion from the first consultation to the last. A nice bloke and very competent in my experience.

Colin Northrop
1630538298
Surgery with minimum invasion, minimum pain and very quick and easy recovery. I would recommend Dr Limbers most highly for his amazing work.


Chris LAMONT
1627005113
I did a great deal of homework before choosing Dr Limbers to do bilateral (two) knee replacement on both my pain ridden knees. I had heard so much conflicting information out in the market place about different surgeons that it was of the utmost importance that I choose well. My excellent results is a true and accurate testament of how accomplished Dr Limbers is at his profession. I recommend him with the highest degree of sincerity. I am walking freely after five weeks from date of surgery. I couldn’t have dreamed of a better result.

Christine Berthelemy
1626568273
Christine Berthelemy
Dr Limbers is very professional and friendly and explained my hip replacement in full detail. I was booked for surgery within 4 weeks.
The care and attention I received from my first appointment to the 6 week follow up was excellent. The procedure and all the staff at Gosford Private were amazing Doctors, Nurses Physio and the lovely catering staff could not be more caring and attentive. The food was plentiful and extremely enjoyable. Facilities were very clean and well looked after.
Dr Limbers office staff were very pleasant and helpful at all times.
I would recommend Dr Limbers to anyone looking for an orthopaedic surgeon he is a very special specialist!
Dr Limbers is very professional and friendly and explained my hip replacement in full detail. I was booked for surgery within 4 weeks.
The care and attention I received from my first appointment to the 6 week follow up was excellent. The procedure and all the staff at Gosford Private were amazing Doctors, Nurses Physio and the lovely catering staff could not be more caring and attentive. The food was plentiful and extremely enjoyable. Facilities were very clean and well looked after.
Dr Limbers office staff were very pleasant and helpful at all times.
I would recommend Dr Limbers to anyone looking for an orthopaedic surgeon he is a very special specialist!

Bill Donaldson
1624340854
Great surgeon who is friendly and patient focused. Needed to have both my knees replaced due to Osteoarthritis. Six weeks post op, no pain, walking 30 mins a day and 10 mins on exercise bike. Will only get better from here. Thanks Dr Limbers

Nicholas Unkovich
1624239349
Fantastic and couldn’t recommend anymore highly. Was very happy to be seen by John. Was made to understand process and recovery. Everything well and tracking strong so far.

Phillip Deal
1622943190
My experience with DR Limbers. I found him to be very good he came highly recommended from my GP. I had both knees replaced at the same time hesitant at first but after having the operation from Dr Limbers recommendation to have both done at the same time has been a huge success for me. I would highly recommend Dr Limbers to anyone who is looking down the barrel of 1 or both knees to be replaced.

Blain Vandersteen
1622519549
I didn't like the advice, but looking back even a few hours it's definitely the right call. Good guy, very knowledgeable from all accounts of other people who have seen him.

anthony spencer
1612486042
I have had four operations with Dr John limbers. All were done in a Higley professional manner. My recovery time and pain relief was in a minimal time. I strongly recommend Dr John Limbers and his team to everyone.

Norma Cadwallader
1607497942
I had a total hip replacement 7 weeks ago and am delighted with the results. I was walking with a stick on the day after the operation. Back doing aqua aerobics after 5 weeks and am now walking with confidence although I use my stick outside. The whole experience has exceeded my expectations. Dr Limbers and his team made sure I was well informed with additional material to refer to. A slight blip (a sore throat) was dealt with sensitively and a new date for my operation was given within 3 weeks of the first date. I would highly recommend Dr Limbers and his team.

Michael Crowe
1602648281
I had a full knee replacement 6 weeks ago, after years pain, and found the whole experience impressive. I was walking unassisted within a week and plan to return to work on week 7. I can thoroughly recommend Dr Limbers and his team as well as the 360 physio program which assisted in my recovery.

allan curtis
1600942683
Twelve years after my first TKR, you can understand my apprehension when
I was told I needed a second TKR. The SAN introduced me to Dr.John Limbers and he recommended the MACRO ROBOTIC TKR. Allelujia!! what a difference 12 years can make. Different Surgeon and different Method. Consequently, a quicker recovery and faster mobility.
Thanks so much to the professional skills endowed to Dr. J. Limbers and his friendly and jovial manner. Will certainly recommend him to my dear and suffering friends. Anita Curtis
I was told I needed a second TKR. The SAN introduced me to Dr.John Limbers and he recommended the MACRO ROBOTIC TKR. Allelujia!! what a difference 12 years can make. Different Surgeon and different Method. Consequently, a quicker recovery and faster mobility.
Thanks so much to the professional skills endowed to Dr. J. Limbers and his friendly and jovial manner. Will certainly recommend him to my dear and suffering friends. Anita Curtis

bruce gibbs
1598962119
I suffered for many years with knee pain, that affected my quality of life.
Finally, in desperation, I asked my very helpful GP Dr Howard Oxley to refer me to the best Orthopedic Surgeon he knew in my area ! My GP did a great and wonderful service in referring me to Dr John Limbers !
My experience right from my first interview with Dr John Limbers, last interview and all surgical procedures in hospital was 'first class'.
Initially, Dr Limbers demonstrated the Mako Robotic knee surgery procedure, and asked me if I would like to take part in the 360 Patient Partner Program he has introduced for patients pre and post surgery physiotherapy needs.
A wonderful 360 Patient Partner Program physiotherapist Denise Korhonen took me through the 8 week program via virtual video daily exercises and bi-weekly interviews with great care, professional advice. and kind attention. The program also supplied a free Garmin watch, and an inflatable knee unit for applying ice packs post surgery.
I can highly recommend the 360 Patient Partner Program Dr Limbers advises to patients, as well as sincere gratitude to the nurses and physiotherapists of Gosford Private Hospital who looked after me so kindly and professionally.
The result ? At 78, after 6 weeks, I am now walking 'Prince' my precious Welsh Corgi over 4,000 steps a day, including gardening, and daily duties all without pain, and without a stick !!
Thank you Dr John Limbers, Denise Korhonen, and GP Dr Howard Oxley from a very satisfied patient.
Harold Gibbs JP
Finally, in desperation, I asked my very helpful GP Dr Howard Oxley to refer me to the best Orthopedic Surgeon he knew in my area ! My GP did a great and wonderful service in referring me to Dr John Limbers !
My experience right from my first interview with Dr John Limbers, last interview and all surgical procedures in hospital was 'first class'.
Initially, Dr Limbers demonstrated the Mako Robotic knee surgery procedure, and asked me if I would like to take part in the 360 Patient Partner Program he has introduced for patients pre and post surgery physiotherapy needs.
A wonderful 360 Patient Partner Program physiotherapist Denise Korhonen took me through the 8 week program via virtual video daily exercises and bi-weekly interviews with great care, professional advice. and kind attention. The program also supplied a free Garmin watch, and an inflatable knee unit for applying ice packs post surgery.
I can highly recommend the 360 Patient Partner Program Dr Limbers advises to patients, as well as sincere gratitude to the nurses and physiotherapists of Gosford Private Hospital who looked after me so kindly and professionally.
The result ? At 78, after 6 weeks, I am now walking 'Prince' my precious Welsh Corgi over 4,000 steps a day, including gardening, and daily duties all without pain, and without a stick !!
Thank you Dr John Limbers, Denise Korhonen, and GP Dr Howard Oxley from a very satisfied patient.
Harold Gibbs JP

Maxwell Moore
1598341554
I have had three operations with John limbers. Each operation has had exceptional results. The latest being a total knee replacement.which has had great results. I can highly recommend John from the beginning to the end. The other two operations involved pins and plates and I would not know there was ever anything wrong.

Ross Walker
1594170084
I am a medical doctor & researched the top surgeons for my knee replacement. My experience with Dr Limbers has been first class from my initial consultation, the operation & with his ongoing care. I am now over 6 weeks post op & feeling stronger with minimal pain. I would highly recommend his extraordinary service.

Sue O'Malley
1593737865
I had both hips replaced (10 weeks apart) by Dr Limbers and have had excellent results with both. Additionally, the recovery time was very short.
Dr Limbers is not only a superior surgeon but he is also conscientious, visiting every day while I was in hospital. I now have two perfect hips that will last me the rest of my life. Highly recommended!
Dr Limbers is not only a superior surgeon but he is also conscientious, visiting every day while I was in hospital. I now have two perfect hips that will last me the rest of my life. Highly recommended!

Martin Christopher Francis
1593553285
I was really impressed with the Dr Limbers and the way he addressed my meniscus injury. I had this injury which required surgery. I feel so good after the surgery and cannot thank him enough.
I was initially advised by someone else that I would not require surgery after reviewing my MRI and would be fine after a few weeks, 8 weeks had past with no change to the pain in my leg and knee area. Thankfully a visit to Dr Limbers saved me the agony or continuing with the injury, two weeks later the surgery was carried out and I am a new man ! 👏🏼👏🏼👏🏼 Thank you Sir !
I was initially advised by someone else that I would not require surgery after reviewing my MRI and would be fine after a few weeks, 8 weeks had past with no change to the pain in my leg and knee area. Thankfully a visit to Dr Limbers saved me the agony or continuing with the injury, two weeks later the surgery was carried out and I am a new man ! 👏🏼👏🏼👏🏼 Thank you Sir !

June Beeston
1584152003
I recently had my right knee replaced by Dr John Limbers, and found the whole procedure from beginning to end highly professional. Dr Limbers “Robotic Procedure” replaced my knee in 1 hr. Pain management was excellent, I had minimal swelling, and I was up and moving around much faster than I thought would be possible - & I’m 86 years young -:). Within 4 weeks, having followed my exercise/physiotherapy plan I’m walking up & down steps independently (no walking aid
required or assistance). I can’t speak highly enough of Dr
Limbers & his knee replacement procedure. I found him to be a very caring man, & his staff happy & caring which helped me feel more relaxed and supported through a rather anxious time.
required or assistance). I can’t speak highly enough of Dr
Limbers & his knee replacement procedure. I found him to be a very caring man, & his staff happy & caring which helped me feel more relaxed and supported through a rather anxious time.

Paul Thornett
1582265395
I had a Total Knee Replacement with Dr Limbers nearly 7 weeks ago, and found the experience much more pleasant than I had expected. Before the operation he explained the process to me very thoroughly, also referring me to a pre and post-op physiotherapist, at no cost to myself, who monitored my progress each day via a video link, setting and tailoring to my specific needs a very useful exercise regime.
I have no hesitation whatever in recommending Dr Limbers, whom I found to be highly professional, courteous and very likeable.
I have no hesitation whatever in recommending Dr Limbers, whom I found to be highly professional, courteous and very likeable.

Jennifer Mifsud
1582099927
I found Dr Limbers to be very friendly and professional when he explained the Mako Robotic Hip Replacement procedure that he performed on me last month. I recommend Dr Limbers to anyone considering this operation.

Richard May
1581986329
Hi, I am 67 and I felt I should share some info for others who may be considering a TKR.
If you are living with knee pain and restricted movement related to the deterioration of the knee joint, I was. I was in considerable pain and it was affecting my movement and quality of life even driving and sleeping. I was referred to Dr Limbers and before attending I did my research
If you are living with knee pain and restricted movement related to the deterioration of the knee joint, I was. I was in considerable pain and it was affecting my movement and quality of life even driving and sleeping. I was referred to Dr Limbers and before attending I did my research

Denise Conway
1581920586
Dr John Limbers what a Surgeon. I had a Mako Robitic Hip Replacement. All steps were explained. Fantastic that a Surgeon keeps up to date with new technology. 2 days in Hospital back to work in 1 week on light duties. All questions were answered regarding aftercare, he makes you feel at ease that nothing is a silly question and you are important. What a Credit to your profession. Keep up the good work. Thankyou Denise

Jo Jo
1581140838
I saw Dr Limbers for my foot injury, he ordered a scan and referred me to one of the best nerve graft surgeon in RNSH. Thanks Dr Limbers.

Lesley Coote
1580714122
I went to Doctor John Limbers for a total knee replacement in November 2019. Today marks twelve weeks since the surgery and I am happy to say that I am pain and medication free. I have returned to full time work and am enjoying experiences that we often take for granted such as a walk along the beach or a trip to the shops. Prior to surgery such ventures were met with pain and a high level of personal frustration, not to mention lots of medication to control the constant pain.
I found Dr Limbers to have a professional and caring nature. From my very first consultation, to his daily visits while I was in hospital and then my follow up consultation. I felt my needs were valued and supported with every question I put to him answered in detail.
I must also add that my anaesthetist, Dr Gray certainly put my mind at ease giving me a bit of a pep talk when I informed him of my ‘possible unrealistic’ fear of the anaesthetic process. The reception girls were wonderful and very friendly and the staff at Gosford Private, in the ward and in rehab were exceptional in their care and professionalism.
All round Dr Limbers and his team made my journey as professional and comfortable as possible and I would highly recommend them for orthopaedic surgery.
I found Dr Limbers to have a professional and caring nature. From my very first consultation, to his daily visits while I was in hospital and then my follow up consultation. I felt my needs were valued and supported with every question I put to him answered in detail.
I must also add that my anaesthetist, Dr Gray certainly put my mind at ease giving me a bit of a pep talk when I informed him of my ‘possible unrealistic’ fear of the anaesthetic process. The reception girls were wonderful and very friendly and the staff at Gosford Private, in the ward and in rehab were exceptional in their care and professionalism.
All round Dr Limbers and his team made my journey as professional and comfortable as possible and I would highly recommend them for orthopaedic surgery.

LYNETTE HINTON
1579835248
Dr Limbers operated on me on 7/12/19 with a full hip replacement I found him to be very professional and very genuine kind Dr and very happy with my new hip thank you Dr Limbers

Josh McMahon
1571120368
A few months ago Dr Limbers completed my ankle surgery - he was, and continues to be, excellent. From the beginning he was open and clear about the process, he supported me through my surgery and continues to throughout my recovery. He is an excellent surgeon - if i ever have the need I would absolutely return to Dr Limbers.
×